TOTAL FEMALE FITNESS
You’ve done the workouts.
You’ve tracked the food.
Maybe you've even tested your hormones.
You think you're doing everything “right.”
But you're still stuck, puffy, moody, bloated and tired af.
It’s not in your head. The disconnect that you feel is real.
It’s your total metabolic health.
At Total Female Fitness, we recognize that the way you feel and perform is much more than any one thing, but how all these things work together to create your individual constitution.
The years leading up to menopause create major hormonal shifts and new challenges for women on their health journey. Which is why our programs are based on your biofeedback, lab work, physical assessment, nutrition, and workouts to provide functional support for women who are ready to stop spinning in and start seeing real results.
Fully customized programs that focus on my key strategy that has helped hundreds of women just like you.
This isn't another cookie-cutter plan.
Lab Based Strategy
No more guessing! We test your hormones, stress markers, and more to uncover what’s REALLY going on.
Customized Nutrition & Training Plans
Based on individual biofeedback. YOUR body, YOUR goals, and YOUR season of life.
Weekly 1:1 Check-Ins
Assessments and the support you need to learn and implement effectively. Obstacles will come, but you're not alone. Together we will troubleshoot and adapt strategies with your progress so you're never left hanging on your plan.
Lifestyle & Supplement Protocols
From sleep to stress to gut health, we address the full picture.
Just because your symptoms are common, doesn't mean they're normal. Stop ignoring the signs and start feeling better.
Low energy. Belly fat that won’t budge. Chronic fatigue. Low lidido. Night sweats. Mood swings.
You’ve been told “you're just getting older.”
We call BS!
It’s time for a different approach—one that actually works
for where you’re at in life.
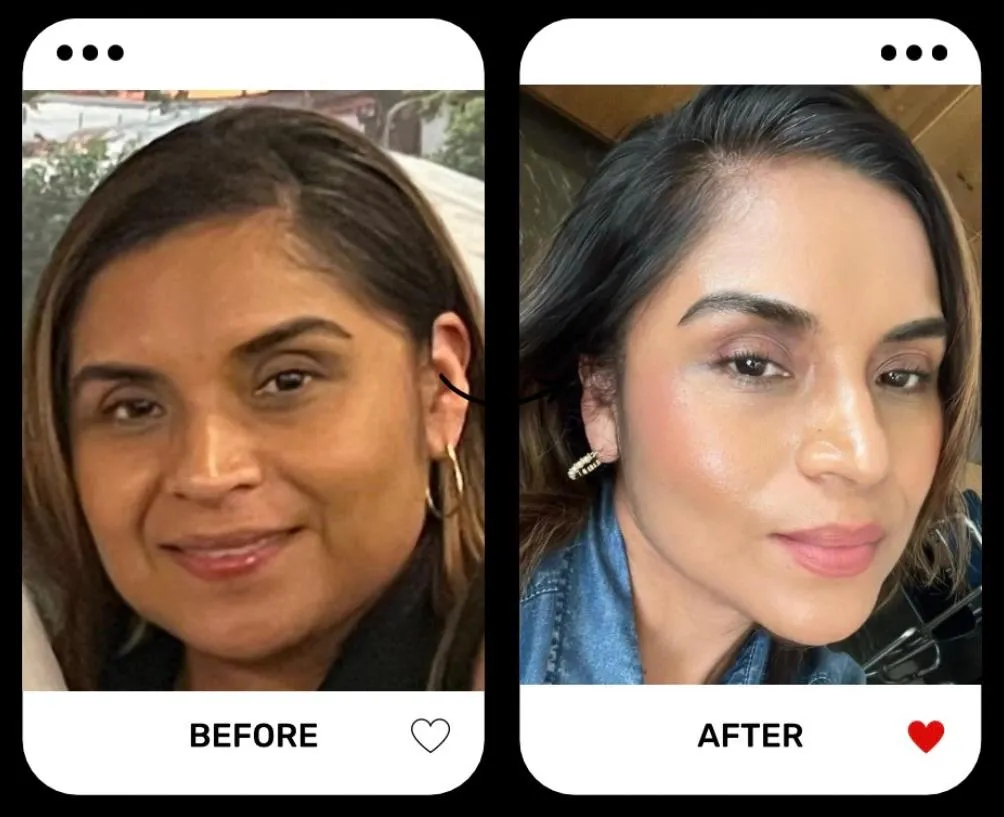
TESTIMONIALS